
Nature of the disease
Hidradenitis suppurativa/acne inversa (HS) is a multifactorial, chronic, inflammatory, recurrent disease of the skin appendages, which can lead to severe scarring and disability and can cause a significant, but greatly underestimated, burden on patients. The 1st International Research Symposium on HS, which took place from 30.3 to 2.4.2006 in Dessau, has formulated the following definition of the disease: “HS is a chronic, inflammatory, recurrent, debilitating skin disease (of the terminal hair follicle), that usually presents after puberty with painful, deep-seated, inflamed lesions in the apocrine gland-bearing areas of the body, most commonly the axillary, inguinal, and anogenital regions (Dessauer definition).
Epidemiology
The reported prevalence of HS in older studies ranged widely from 0.03 to 4%. Women are more commonly affected; the male-female ratio is 1:2.7 to 1:3.3. An exception to this is the involvement of the perianal area, where men seem to predominate. HS seems to develop rarely before puberty or after menopause, although the persistence of existing lesions after menopause is not unusual. It was reported that only 2% of cases occur before the age of 11 years. The average age at onset is 23 years.
Clinical findings
HS presents a variable clinical course.
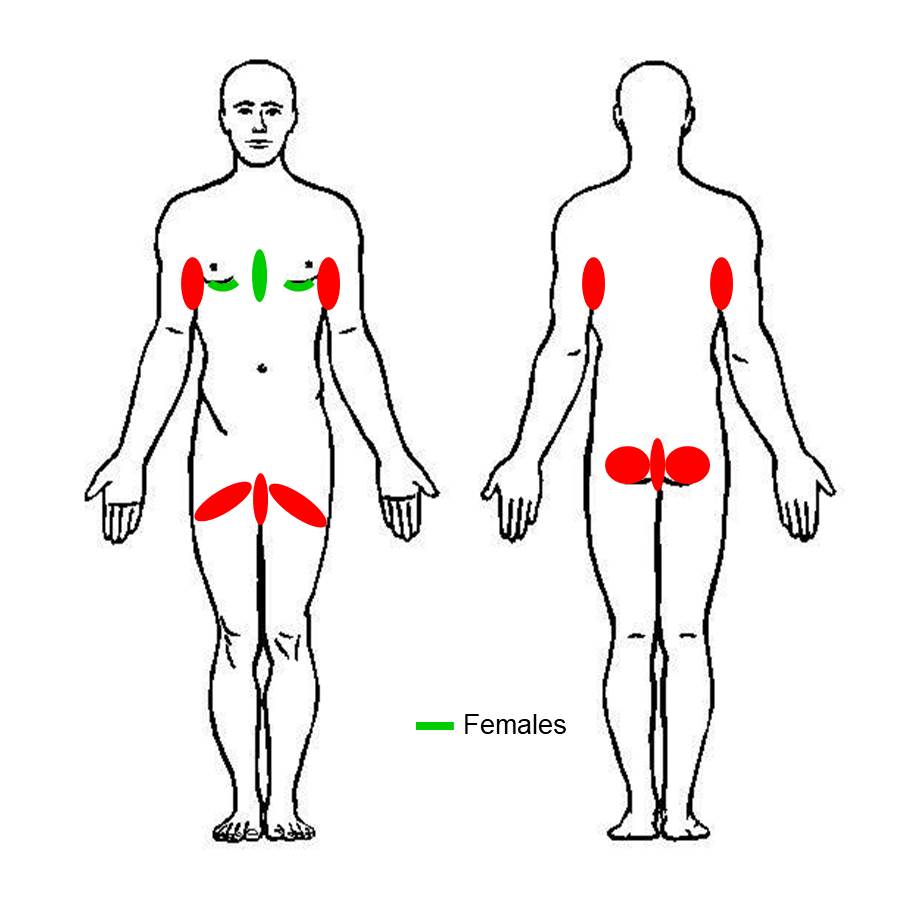
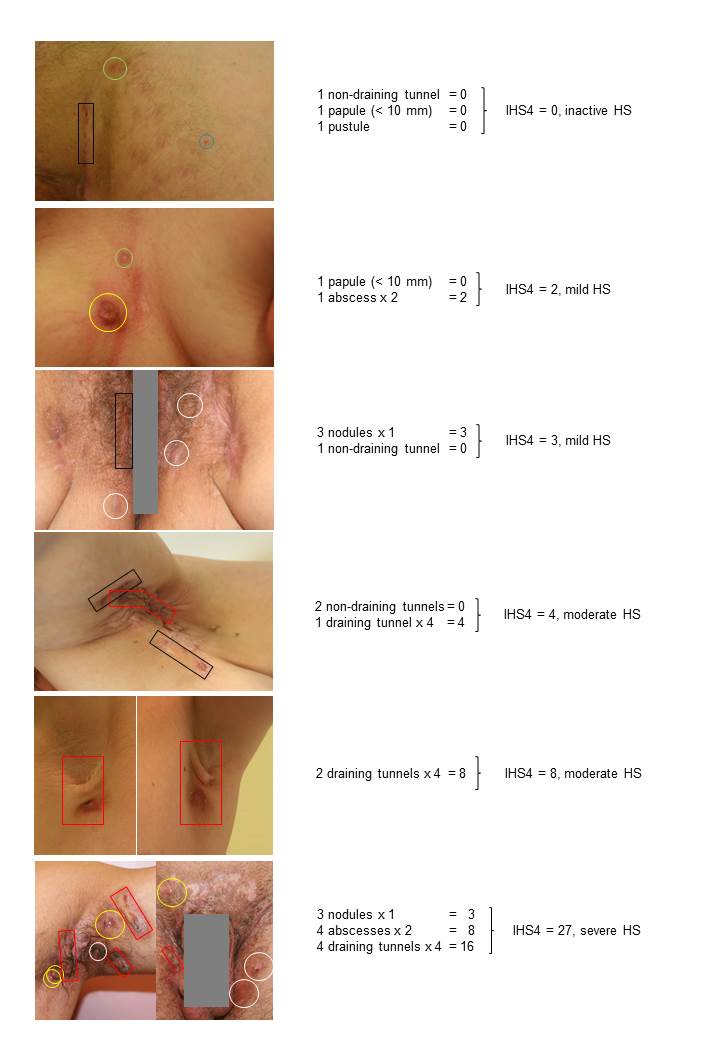
One of the main features of the disease is the intertriginous occurrence, although other areas of skin may also be affected. The affected areas in decreasing order of frequency are: inguinal, axillary, perineal and perianal, as well as the submammary and/or intermammary fold in women, buttocks, mons pubis, scalp, behind the ears and eyelids. Inflammatory nodules, abcsesses, draining tunnels (fistulae, sinuses) are considered active specific HS lesions. The initial transient superficial lesions, namely follicular papules and pustules (folliculitis) are not diagnostic. 23-30% of HS patients are also affected by a pilonidal disease.

HS diagnosis
For such a chronic, debilitating disease, efficient screening of the population in primary care setting to early detect possible HS cases is essential, in order to facilitate early referral. This is reflected in the current long mean time to diagnosis of 7 years. Since HS lacks a specific test, implementation of criteria to be used both in primary care setting and by dermatologists, is of high significance.
Recent evidence suggest that a positive reply to the following question could identify HS patients with a sensitivity of 90% and a specificity of 97%: “Have you had outbreaks of boils during the last 6 months with a minimum of two boils in one of the following five locations: axilla, groin, genitals, under the breasts and other locations (not specified), e.g. perianal, neck and abdomen”. The term boil is used since HS patients usually refer to their lesions with it. Since such a definition is very easy to use in primary care setting, and has shown adequate specificity and sensitivity, it is recommended to be used in such a setting for early identification of patients.
Laboratory markers
No laboratory markers exist. HS patients with active inflammation may have an increase in the blood cell sedimentation rate or C-reactive protein. At the presence of further signs of inflammation, including temperature increase, a soft tissue infection must be considered and excluded.